
What to expect during a CLM pregnancy
This guide walks families through what to expect during pregnancy if their baby has been diagnosed with a congenital lung malformation like CPAM/CCAM, BPS, CBA or CLE/O.
Medically reviewed by Marisa Schwab, MD
Written by Emily Lake, PhD
Last updated 06/02/2026
Introduction
Receiving a congenital lung malformation diagnosis like CPAM/CCAM or BPS during pregnancy is a significant experience that can feel really overwhelming. You may now need to travel to multiple appointments, learn for the first time about these rare lung conditions, and navigate a lot of uncertainty, all while you are understandably worried about what this diagnosis means for your baby.
This guide walks you through what to expect during the prenatal experience: from appointments, who will be on your medical team, the monitoring your baby will receive, and the decisions you may face before birth, whether your baby has been diagnosed with CPAM, BPS, CLE, or a hybrid lesion. Every CLM pregnancy is different, and most will progress without major complications. But understanding what your care team is watching for, and why, can help you feel more prepared and more able to advocate for your baby.
Diagnosis
Diagnosis during pregnancy typically happens at a routine prenatal ultrasound scan, normally when the baby is around 20 weeks’ gestation. An ultrasound technician may notice a bright patch on the lungs, which suggests an area of abnormal microcystic or solid tissue, or a dark patch, which suggests a fluid-filled cyst. They may also notice that the heart is in a slightly different place than expected if the CLM is causing what’s called “mass effect” (pushing other structures in the chest). A specialized doctor, called an MFM (Maternal Fetal Medicine), should discuss the diagnosis with you. They may tell you what they can see from the ultrasound and how big the CLM appears to be. They might give you the CVR number, which estimates how large the CLM is in relation to your baby’s head. The size of the lung malformation, and whether it is causing other complications, are more important than the specific diagnosis at this stage (i.e. CPAM vs BPS). In fact, it can be really hard to tell different CLMs apart on ultrasound and even on Fetal MRI! Many families are initially given one diagnosis which is then changed later when the medical team gets more information from imaging.
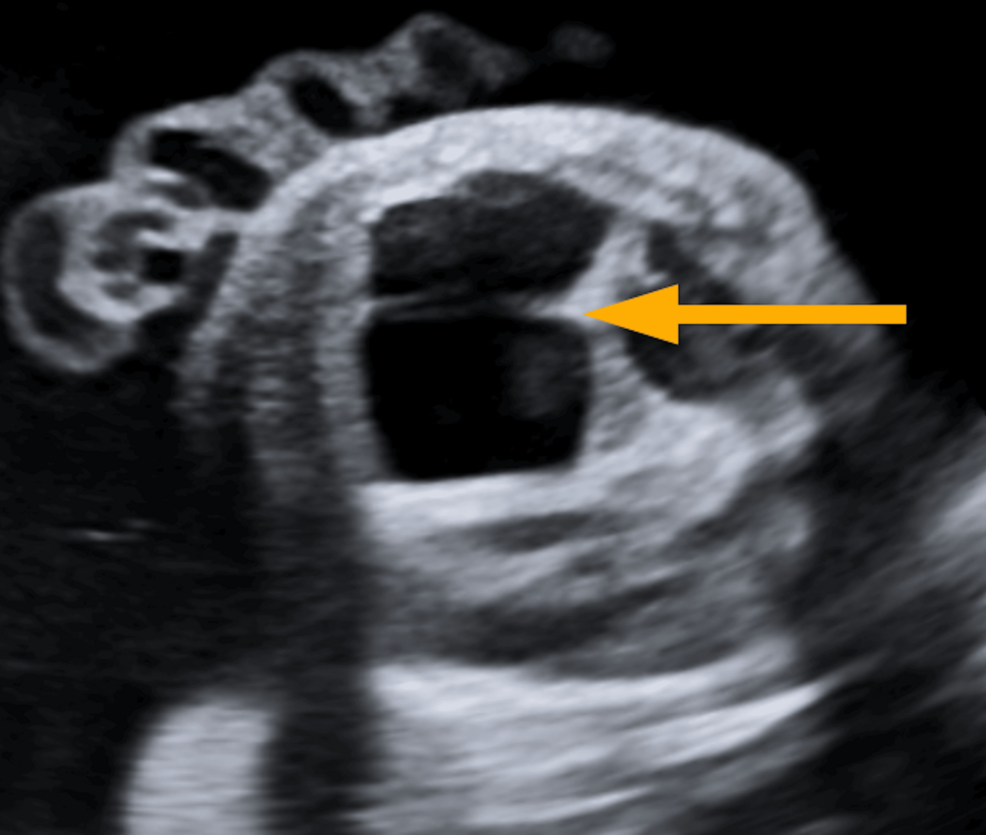
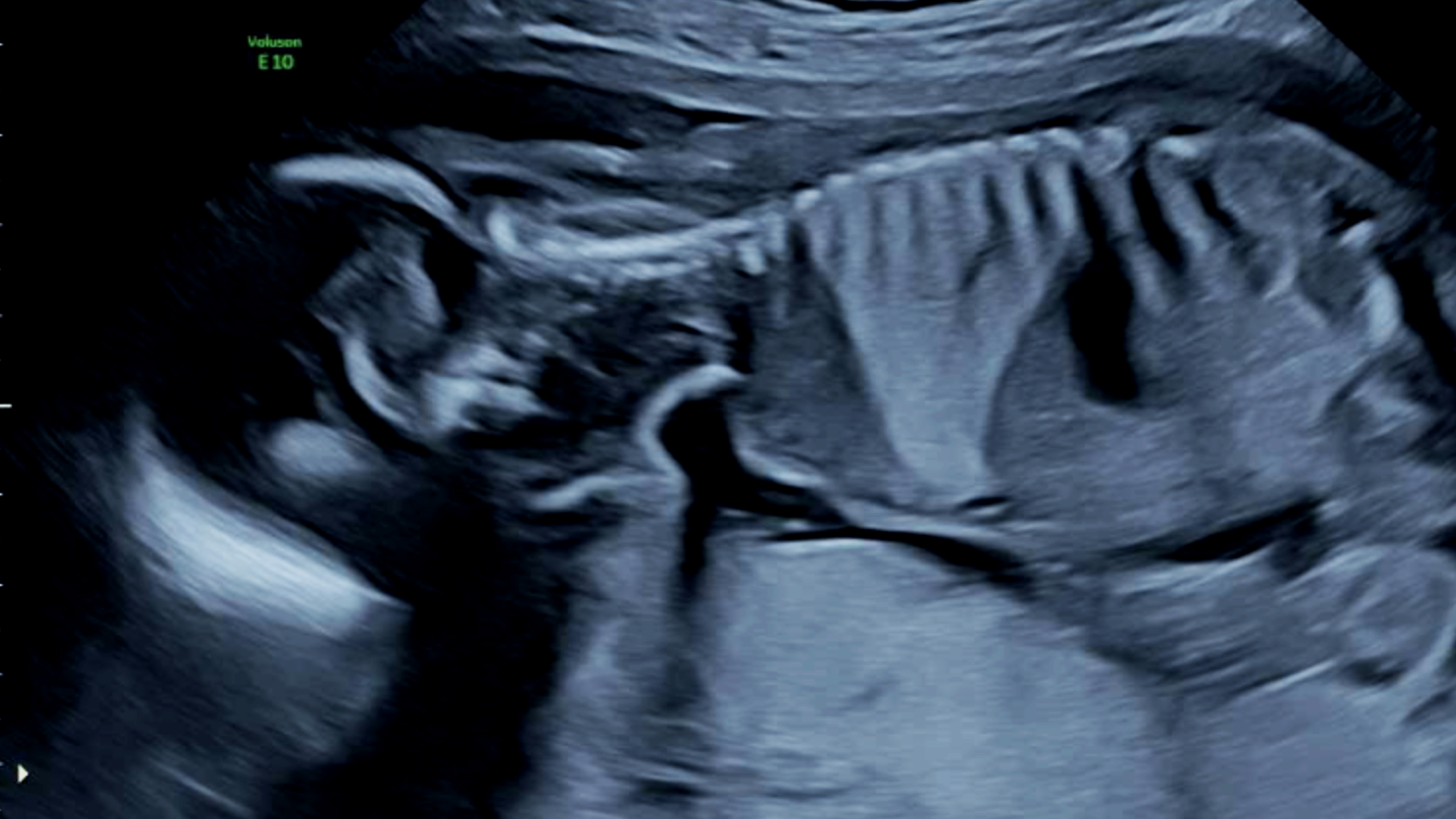
A macrocystic CPAM (left) appears darker than the surrounding healthy lung tissue on ultrasound. A BPS (right) appears brighter than the surrounding lung tissue. Images: (left) Sathian et al (2026) and CLM Society (right).
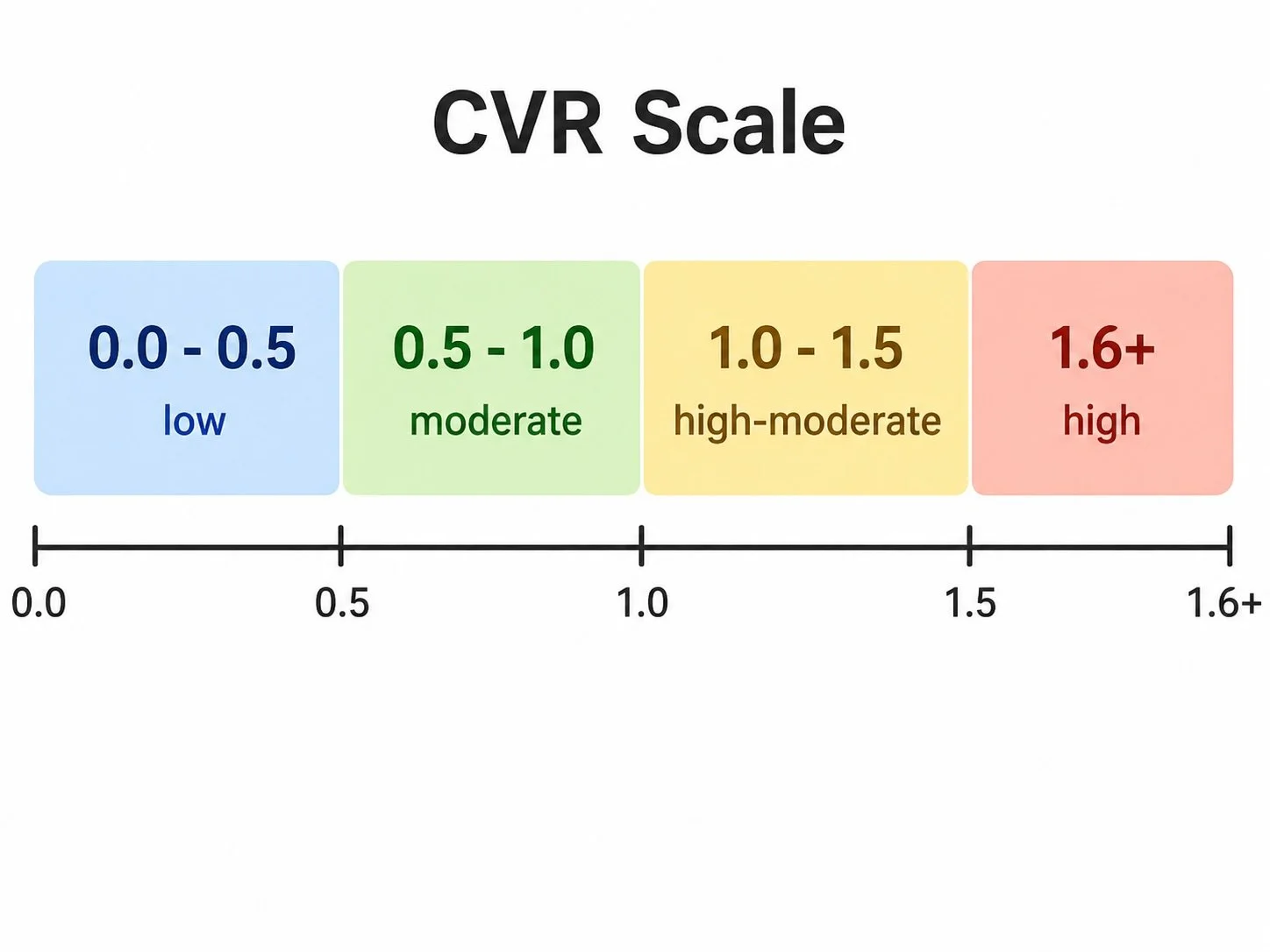
The CVR number
At your prenatal appointments you may be given what is called the CVR number. CVR stands for “CPAM Volume Ratio” and is a way of estimating how big the CLM is in relation to your baby’s head circumference. Even though it has the word CPAM in the title, the CVR is used to measure all congenital lung malformations.
Keep in mind that while it is standard practice in the USA to share the CVR with parents, this is not the case everywhere in the world. Don’t be alarmed if your doctor doesn’t give you the CVR number for your baby’s lesion.
Most lung malformations will be small, meaning the CVR will be well under around 0.5. A CVR between 0.5-1.0 is considered moderate. A CVR over 1.6 is considered high and places the baby at increased risk of dangerous complications, such as hydrops.
Monitoring
The vast majority of CPAM cases are not high risk and will not present serious complications to either you or your baby during pregnancy. But even in low risk CPAM cases, your pregnancy will be more closely monitored than an uncomplicated pregnancy. Your medical team will look at the size and appearance of the CPAM and track its growth over time. You will be asked to come in for ultrasounds more frequently. Depending on the size of the CPAM, this could be weekly or every couple of weeks. In high-risk cases, which are rare, you might have to come in twice a week.
Sometimes a fetal MRI may be carried out during the pregnancy to get a more detailed picture of the CPAM, although this is not offered everywhere or for every case. Where the heart is pushed or compressed by the CPAM, a fetal echocardiogram may be requested by your medical team to get a more detailed look at blood flow and how the heart is functioning.
Ultrasounds can normally be carried out where you were already receiving prenatal care. You will need to go to a specialist hospital for more specialist imaging if it is requested, like a fetal MRI and fetal echocardiogram.
The risks depend on the size, type, and other findings on imaging (such as mediastinal shift and hydrops). Most lung malformations like CPAM and BPS will increase in size between 20 and around 28 weeks gestation, and then will stay the same or decrease in size. The period between 20 and 28 weeks is often the most stressful for families. There may be many appointments to keep a close eye on how your baby is doing and you might feel anxious at each scan.
Your care team
Many different specialists will now be involved in you and your baby’s care.
Depending on where you’re receiving prenatal care, you will be connected to a maternal-fetal medicine (MFM) specialist. This is a doctor who works with pregnant women and unborn babies during high risk and complicated pregnancies. The MFM should understand CPAM and will make sure you and your baby are properly cared for.
A radiologist will take specialized images of your unborn baby during ultrasounds and interpret these findings. They will be looking for how large the CPAM is and whether it shows any characteristics that might change the course of management and treatment, such as whether it appears to be made up of one lesion or many smaller lesions, and whether these appear to be cystic (filled with fluid or air) or solid.
They will also closely look for any signs that the CPAM might be pushing on other organs, such as shifting the heart to the other side of your baby’s chest (mediastinal shift). Doctors will also look for hydrops, which is when fluid builds up in a body’s tissues or organs (such as the lungs, heart, or belly).
Closer to the third trimester you will then likely have a consultation with a pediatric surgeon to understand if they plan to operate, when this would be, and what an operation would look like. You may also ask for a consultation with a neonatologist (the specialist doctors who work in NICUs) to understand what will happen at birth if your baby is symptomatic.

Want to learn more about who works with CLMs?
Our Meet an Expert Q&A series has interviews with medical professionals who work with congenital lung malformations like CPAM and BPS.
High risk cases
Higher risk cases are uncommon. If a baby’s CLM is very large (greater than a CVR of 1.6) they will be watched extremely closely for signs of hydrops or other fetal distress. Hydrops can be dangerous for both mother and baby, so your doctors will watch you very closely. Depending on the size and change of the CLM, your doctors may recommend a treatment during pregnancy.
Prenatal interventions
Maternal steroids (betamethasone) may help shrink microcystic/solid CLMs and can prevent or reverse hydrops in some cases. You may be given multiple doses of steroids.
Thoracoamniotic shunt (a tiny drain placed through the baby’s chest wall into a large fluid-filled cyst) can shrink the size of macrocystic CPAMs.
Fetal surgery and EXIT procedures are rarely considered and carry significant risks.

Have a high risk CLM case?
Connect with one of our trained peer support counselors who understands what this is like. We are an international team of parents who have been through a CLM diagnosis with our babies. We can help you understand your diagnosis, prepare for appointments so you can have better conversations with your care team, and help you navigate your fears and anxieties.