What is BPS?
A guide for families
This guide explains what BPS (Bronchopulmonary sequestration) is and how BPS is managed and treated.
Medically reviewed by Marisa Schwab, MD | Written by Emily Lake, PhD | Last updated 05/04/2026
What is BPS?
BPS stands for bronchopulmonary sequestration. It is the second most common type of congenital lung malformation after CPAM. Like a CPAM, a BPS is a mass of abnormal lung tissue, but what makes it different from CPAM is that it receives its blood supply from outside the lungs, via one or more feeding vessels connected to a different systemic artery. This is commonly but not always the aorta. A BPS does not function as healthy lung tissue.
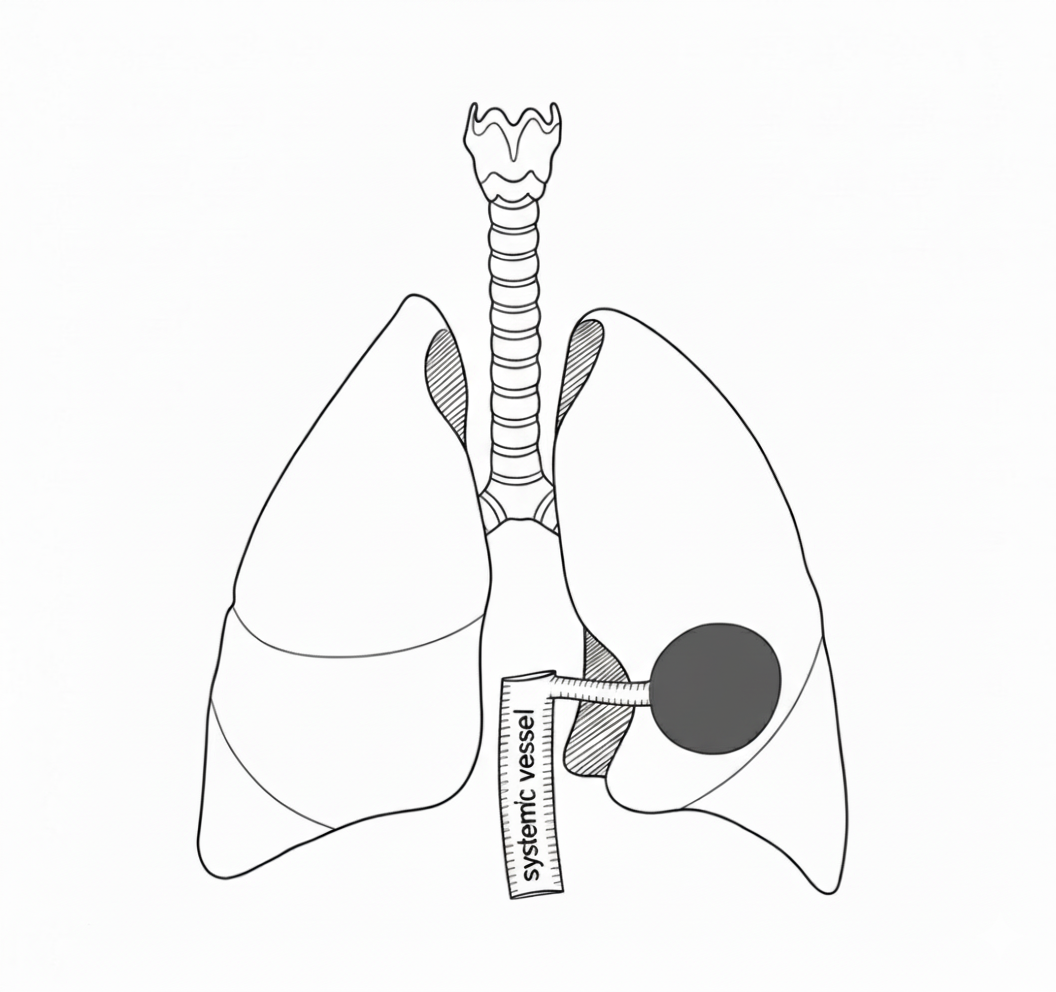
A sketch of a BPS mass (shaded) with a feeding vessel coming from outside the pulmonary system.
CPAM vs BPS
What is the difference between CPAM and BPS? Both are congenital lung malformations and involve an area of abnormal lung tissue that didn’t develop normally early in pregnancy., But there are a few differences between the two. The biggest difference is that a BPS gets its blood supply from outside the lungs, normally the aorta. A BPS therefore has a “feeding vessel” whereas a CPAM does not. A CPAM gets its blood supply from the lungs.
CPAM
a mass of abnormal lung tissue
not cancer
can be microcystic, solid, or macrocystic
blood supply comes from the pulmonary artery, the normal lung blood supply
no feeding vessel seen on imaging
BPS
a mass of abnormal lung tissue
not cancer
almost always solid
blood supply comes from outside the lungs, commonly the aorta
at least one feeding vessel seen on imaging
Mass vs lesion
You’ll see all both of these terms used almost interchangeably when talking about BPS.
Mass: A general word doctors use for an abnormal growth of tissue. Masses can be benign (non-cancerous) or malignant (cancerous). BPS is benign: it is not cancer.
Lesion: A broad medical word for an abnormal area of tissue. With BPS, it means the same thing as “mass” or “the BPS.”
What causes BPS?
The cause of BPS is unknown. Nothing a mother did or didn’t do in pregnancy caused it. These are random malformations that develop in the lungs very early during pregnancy, sometime before the 10th week of gestation.
Why did this happen? Understanding how congenital lung malformations develop
Lung malformations arise from deeply complex biological processes that take place in the earliest weeks of pregnancy, long before most people even know they’re expecting.
Diagnosis
BPS is normally found during a routine prenatal ultrasound scan, usually around 20 weeks of pregnancy. The scan technician commonly notices a bright white patch in the baby’s lungs which suggests an abnormal area of tissue. The external feeding vessel may be seen on the ultrasound, or it might be seen if a fetal MRI is recommended. When the feeding vessel is seen, this means the diagnosis is likely BPS or a hybrid lesion, rather than just CPAM or another CLM.
Imaging before birth gives doctors an idea of what the mass looks like, but it won’t be until a CT scan is done after birth that they’ll have a good idea of whether this is really a BPS or a different type of congenital lung lesion. The CT scan will also give a better idea of the location and characteristics of the BPS. However, it won’t be until after surgery, when the pathologist examines the abnormal lung tissue, that a definitive diagnosis will be given.
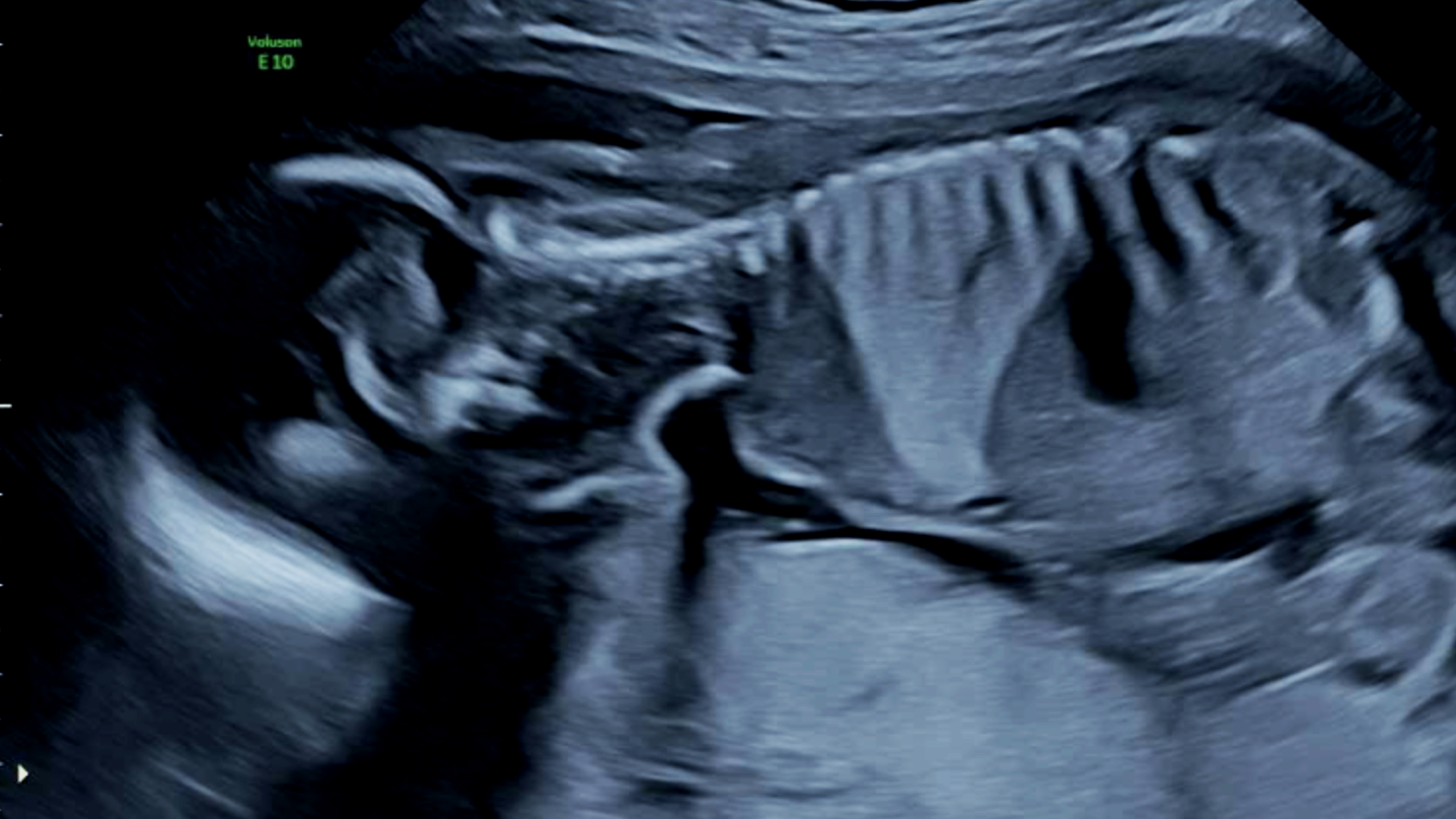
A large BPS mass appears brighter than the surrounding healthy lung tissue on prenatal ultrasound. This baby was diagnosed with an extralobar sequestration. Image: CLM Society
Types of BPS
There are two types of sequestration. The BPS can be intralobar, meaning it is part of a lung lobe (but still with an external blood supply), or extralobar, meaning it is outside of the lung lobes entirely. Intralobar sequestrations are thought to be more common than extralobar sequestrations. In about a quarter of cases, the lung mass will show characteristics of both CPAM and BPS (typically a cystic mass with an external blood supply). These are called hybrid lesions.
Intralobar BPS
a mass of abnormal lung tissue
not cancer
part of a lung lobe
blood supply comes from outside the lung system
more common
can be a hybrid lesion with CPAM characteristics
A sketch of an intralobar BPS mass (shaded), part of the lower left lung lobe, with a feeding vessel coming from outside the pulmonary system.
Extralobar BPS
a mass of abnormal lung tissue
not cancer
outside of the lungs entirely
blood supply comes from outside the lung system
less common
can be a hybrid lesion with CPAM characteristics
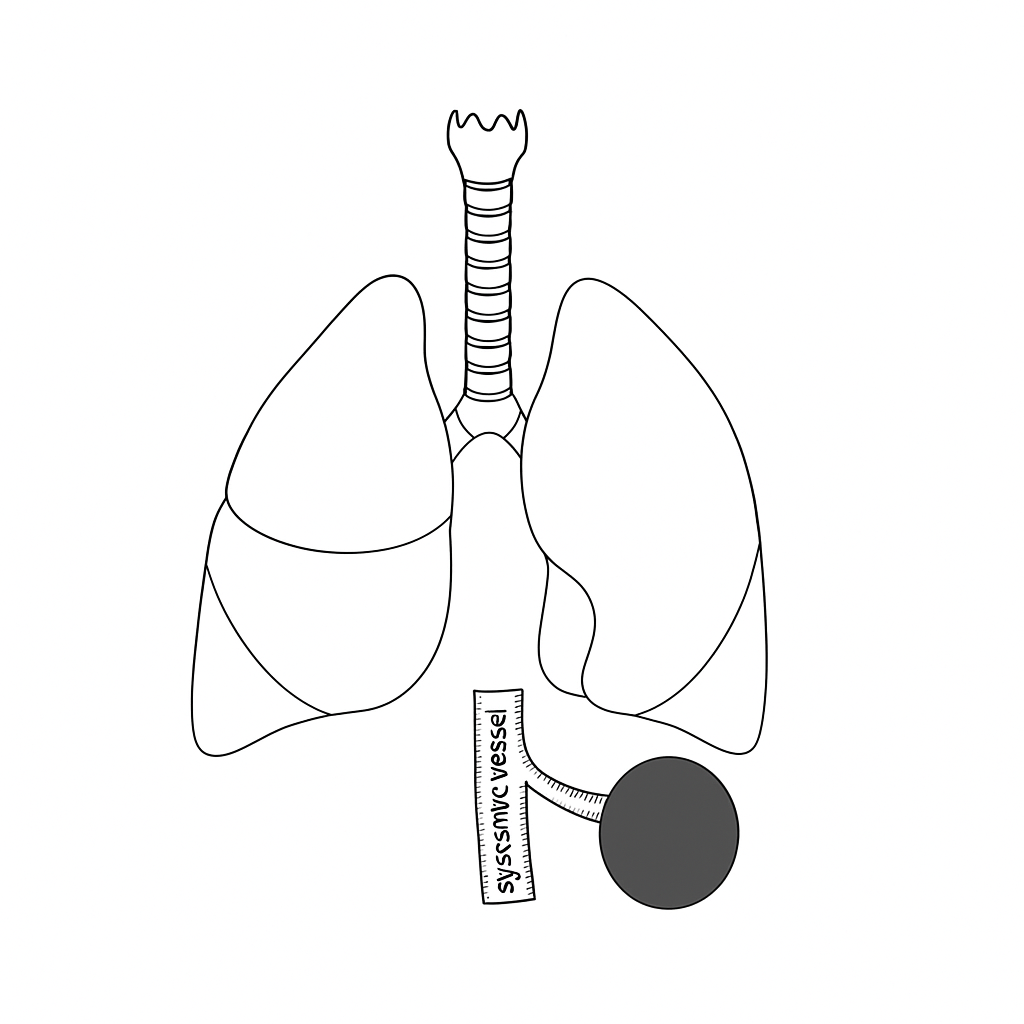
A sketch of an extralobar BPS mass (shaded), not part of the lungs at all, with a feeding vessel coming from outside the pulmonary system.
How rare is BPS?
Congenital lung malformations, including BPS, are uncommon. Estimates for all CLMs are 1 in 2,500 live births. BPS is the second most common congenital lung malformation after CPAM. Intralobar BPS is more common than extralobar BPS. Currently, approximately 70% of babies with a congenital lung malformation are diagnosed before birth.
Cancer risk and BPS
There is not thought to be any risk of cancer from a BPS lesion. There may be an increased risk of cancer with CPAM, and some patients have hybrid lesions, meaning both sequestration and CPAM.

What do we actually know about lung malformations? Q&A with Dr Shaun Kunisaki
We spoke with Dr Shaun Kunisaki—Professor of Surgery at the Johns Hopkins School of Medicine and a Medical Advisor to the CLM Society —about what we actually know, what’s still debated, and what researchers and clinicians are working hard to understand next.
Prognosis
The prognosis for a baby born with BPS is excellent. In the overwhelming majority of cases BPS will not affect a child’s life expectancy or quality of life. In some rarer cases, the BPS presents more serious complications during pregnancy or immediately after birth. In particular, if the BPS grows very quickly, or is very large, fluid can build up in nearby organs. This build up of fluid is a rare but very serious condition called hydrops. When the BPS is more dangerous, the pregnancy must be extremely carefully monitored by specialists. Like CPAM, most BPS lesions will shrink before birth and the majority of babies are asymptomatic, meaning they have no breathing problems before and after delivery. If surgeons recommend that the BPS and affected lung lobe be removed after birth, the healthy lung tissue will expand to fill the space. The vast majority of kids will have no long-term impacts on their health or activity levels.

What to expect during a BPS pregnancy?
A BPS diagnosis during pregnancy is a significant and disruptive experience. Read our guide on what typically happens during a CLM pregnancy in terms of appointments, monitoring, and who will be on your care team.
Management and treatment
There are two main paths for BPS management and treatment. Which one you choose depends on the specifics of your baby’s BPS, the advice of your medical team, where in the world you are located, and what you feel is best for your child.
Elective surgical removal
Most often a thoracoscopic or open lobectomy in later infancy— normally around 3–6 months—even if a child has no symptoms. This means that the surgeon will remove the entire affected lung lobe or, in extralobar cases, the surgeon will normally just remove the sequestration without removing any lung. This is the common treatment path in the USA and usually recommended for all cases of intralobar sequestrations, even if there are no symptoms. The reason this is recommended by most doctors in the USA is to prevent repeated and severe infections (such as pneumonia) for the rest of the patient’s life and make the diagnosis certain. The recovery time depends on whether the operation is done via the open or minimally invasive technique. After a thoracoscopic lobectomy, babies usually recover quickly and spend one or two days in the hospital. If a lobe has been removed, the remaining lung will expand and grow to compensate for the removed lobe, and most children will have the same lung function as someone who didn’t have lung surgery as a baby. They’ll be able to do all the activities and sports they want when they grow up.
Careful observation (“watchful waiting”)
Scheduled check-ins and regular imaging. This is the common treatment path for patients with asymptomatic BPS (especially extralobar sequestrations) in Canada, Australia, and many European countries. If symptoms develop—recurrent chest infections, wheezing not explained by common causes, or a spontaneous pneumothorax—surgery is then usually recommended.